Join Our Advocacy Network and Be Part of the Change
Join our Grassroots Network
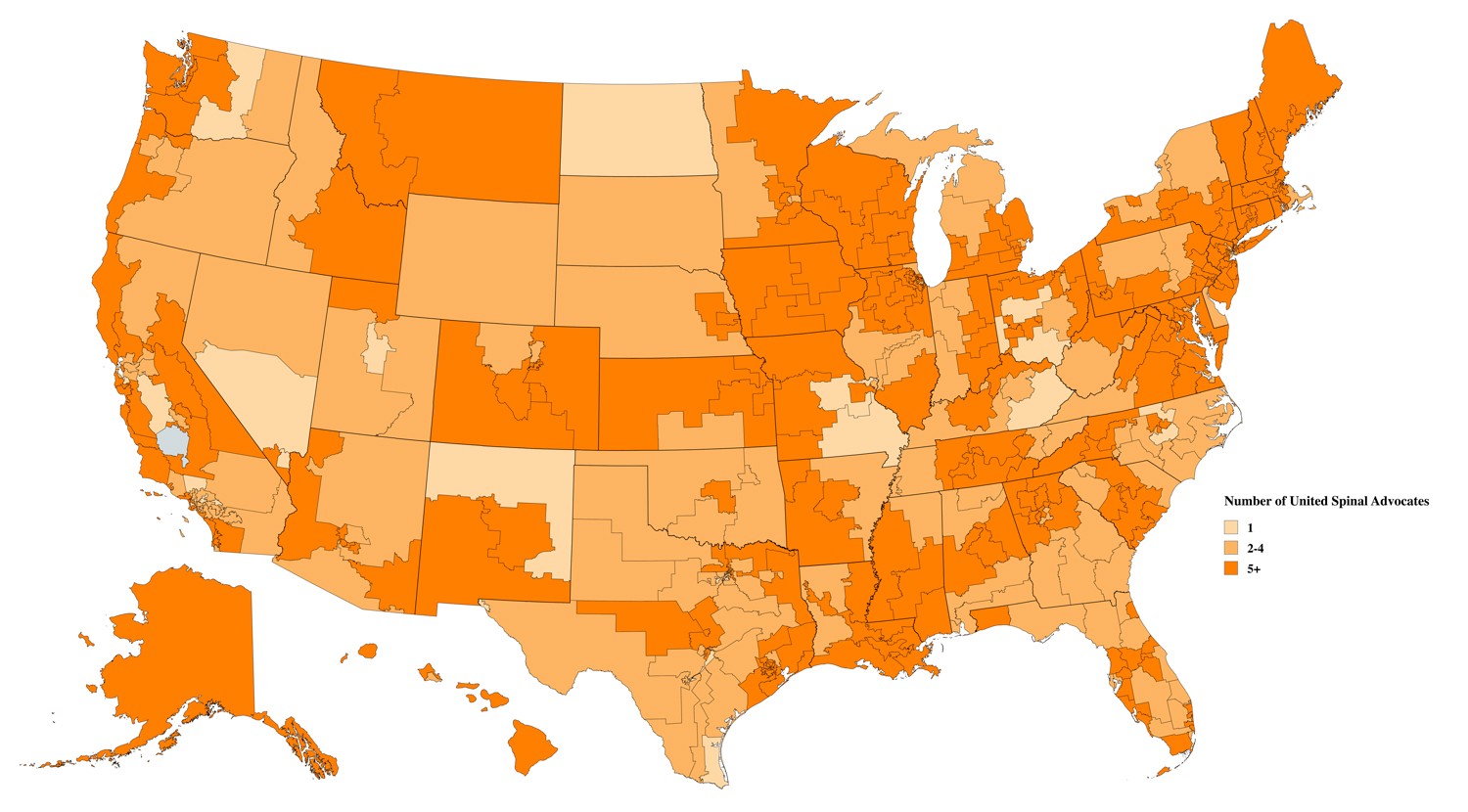
Areas shaded in orange = Districts represented by at least one United Spinal advocate
Help us paint this map a brighter orange by signing up to represent your legislative district as a member of our Grassroots Advocacy Network. Only registered advocates are eligible to attend our Roll on Capitol Hill and Virtual Advocacy Days.
Questions/Help?
Please keep the Advocacy and Policy teams informed of any challenges that you may have or any help that you may need. Don’t hesitate to reach out to the Advocacy Team at advocacy@unitedspinal.org or the Policy Team at policy@unitedspinal.org.
Don’t miss our Advocacy Live conversations every third Tuesday!
Choose 1 pm Eastern or 5 pm Eastern



Advocacy Video Archives


Advocacy Blog Posts
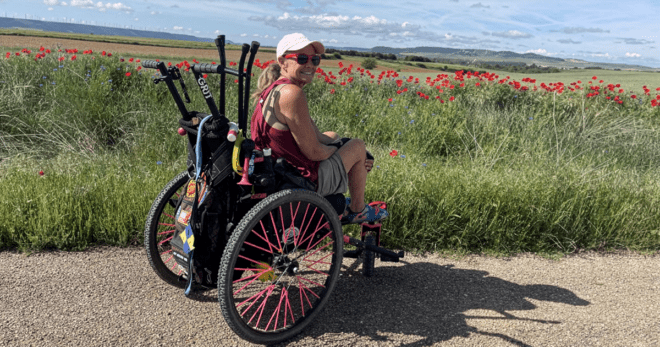
What One Wheelchair User’s 500-Mile Camino Journey Teaches Us About Access and Advocacy
United Spinal Outdoor Working Group member Kim Harrison shares her triumphant 500-mile journey across Spain.

Advocates Urge More Parking Access for All, Challenge Florida Law Impacting Disability Spaces
The complaint challenges the Expectant Mother Parking Permit which allows for parking in disabled spaces.

Meet an Advocate: Allaina Humphreys
Allaina Humphreys discusses her advocacy roles, her mission-driven design studio and the belief that accessibility benefits everyone.

How to Advocate for Better Accessibility at Festivals and Other Public Venues
I bought ADA tickets for a concert only to show up and discover they’d put the wheelchair seats on an awkward sloped hill with terrible sight lines...

Expanding Access to Wheelchair Accessible Vehicles
35 years after the signing of the ADA, millions of people with disabilities still face significant disadvantages when it comes to accessible transportation.

Meet an Advocate: Sled Hockey Athlete and Strawberry Researcher Monica Quimby
Monica Quimby served as Ms. Wheelchair Maine, is a member of the Team USA para hockey team and worked as a biology professor. She shares her story with United Spinal.
Thanks to Our Advocacy & Policy Partners: